

Introduction: In the present era due to the usefulness and availability of apps, games, information, and entertainment, mobile usage has become habitual. Studies have found that mobile phone dependency is associated with an unhealthy lifestyle, extrovert or neurotic personality traits, and maternal affectionate constraints in childhood. Objectives: The objective of this study is to estimate the prevalence of mobile phone dependence among adolescents and assess the relationship between mobile phone dependence and depression among them. Materials and Methods: It is a cross-sectional study conducted among late adolescents and early adults. Data regarding the sociodemographic details, mobile phone dependence, and the factors influencing it were collected using the standardized pretested semi-structured questionnaire. Results: Among 701, majority of the participants (99.7%) were using mobile phones, and among them, about 43.4% of the study participants had mild, 29.1% had moderate, and 4.4% had severe mobile dependence. It was observed that 56% of them had normal, whereas 4% of them had extreme and 2% had severe depression, but no significant association was found between mobile dependency and depression.
Introduction |
The usefulness due to the availability of apps, games, information, and entertainment usage of mobiles has become habitual in the present era.[1] Mobile phone is among the most prominent kinds of Information and Communications Technology and is probably also the one that has shown the most spectacular development during the past few years about technological innovations, social impact, and general use by the majority of the population.[2] A recent global survey revealed that 98% of the Indians sleep with their devices and 57% of Indians cannot live without their android phone.[3] As per the annual Global Mobile Market Report, 2019 India ranks the second for android phone users with 345,916,000 smartphone users.[3] Android phone addiction is an enormous problem already, but it is likely to grow even more common due to the rising demand for and access to the handsets. Mobile phones are said to be the new epidemic of this century and medical students are no exception to it. On one side wherein the mobile phones are helpful in their study purpose, they also face the likelihood of a possible addiction liability to mobile phones. New operating systems such as android and the applications relevant to medical study are helpful, but on the flip side, mobile phones pose a threat in terms of psychological dependence.[4]
The increase in demand for digitally driven interpersonal mass communication over the last decade has fueled the efficient development of cell phone apps. In addition to being a means of communication and having rapidly spreading use worldwide, mobile phones, in particular the new generation of smart mobile phones, are technological tools for offering many functions, such as providing short message service to users, taking photos, playing games, using the Internet, connecting to social networks, providing navigation services, having a video player functionality, watching TV, and shopping.[5] Recent studies have shown that cell phone dependence is linked with an unhealthy lifestyle and extrovert or neurotic symptoms.[6],[7] Today, people have mobile phones with them all the time and use them to organize and manage every moment of their life, from work to free time. Previous studies on Internet use suggest that excessive Internet use may be associated with subjective distress, loneliness, and social disinhibition.[8]
Epidemic continues to grow among college youth and teenagers and teenagers fall right behind adults and most adolescents are addicted to smartphones.[9] The dramatic growth is driven by a desire among youth to stay connected and has instant access to social-networking sites. Mobile phone addiction has serious implications for health. Headache found to be the most common symptom followed by irritability/anger. Other common mental symptoms included the lack of concentration and poor academic performance, insomnia, and anxiety. Among physical symptoms, body aches, eye strain, and digital thumb were found to be frequent. Accidents are caused due to the use of cell phone while driving.[10] Mobile phone has become a vital element for every person, but it is the reason for addiction also. With this background, this study was undertaken.
Objectives
- To assess mobile phone dependence among adolescents and early adults
- To assess the association between mobile phone dependence and depression.
Materials and Methods |
A cross-sectional study was conducted for duration of 5 months. Purposive sampling was adopted. Students of various disciplines (medical, pharmacy, and dental) under the university were included in the study. Students belonging to all the academic years in the respective disciplines were included in the study. A total of 950 students (dental college 400, pharmacy college 300, and medical college 250 students) were planned to be included in the study initially, but only 720 students were present on the day of data collection which included 308 dental students, 228 pharmacy students, and 184 medical students. While the students who had android mobile phones were included in the study, students who were absent on the day of data collection and who did not consent were excluded. Ethical clearance was obtained from the Institutional Ethical Committee, and informed consent was obtained from the study participants before the process of data collection.
Data regarding the sociodemographic details, mobile phone dependence, and the factors influencing, it was collected using a pretested semistructured questionnaire. The questionnaire included the four components: sociodemographic details, mobile phone-dependence questionnaire (MPDQ), factors influencing mobile phone dependence, and scale to measure depression (Beck’s Depression Inventory-2 Scale).
Mobile phone dependency was assessed using a self-rated questionnaire. It includes 22 items, each response being rated on a Likert scale with continuum option as completely disagree, disagree somewhat, neutral, agree somewhat, completely agree, scored on a five-point scale ranging from 0 to 4, respectively. Scores for each item were then summed to provide a quantitative overall mobile phone dependence score. Depending on the overall score, mobile phone dependence was categorized as no dependence, mild dependence, moderate dependence, and extreme dependence.
Beck Depression Inventory-2 is a 21-item self-report inventory used for the assessment of depression. Each item is rated on a 4-point scale ranging from 0 to 3. The maximum total score is 63. Once the scores were obtained, depression was graded into 6 grades which included normal, mild mood disturbance, borderline clinical depression, moderate depression, severe depression, and extreme depression.
The collected data were entered in Microsoft excel and were analyzed using the SPSS version 24 (IBM, Armonk, NY) (licensed to the institution). Descriptive statistics such as percentage, mean, and standard deviation were applied. Inferential statistical tests such as Chi-square tests were applied for testing the association between sociodemographic variables and depression with mobile dependency. P < 0.05 was considered statistically significant.
Results |
Among the total 720 students, 19 of them had missing data and hence were discarded. The analysis was done for the remaining 701 responses. Among them, 99.7% of the students had mobile phones. The mean age of the study participants was 20 ± 2 years, with a minimum age of 17 years and a maximum of 24 years. Out of the total respondents, 37.4% were male and 62.6% were female. Three hundred and three (34.1%) were from dental, 223 (31.8%) from the pharmacy, and 176 (25.1%) from the medical course. Majority of the study participants, i. e, 80.6% (565) belonged to nuclear families followed by 11.7% (82) from the joint family and 7.7% (54) from three-generation families. Majority of the participant’s mothers, i. e, 42.8% (300) had completed PUC/diploma and 25.4% (178) of them were graduates, and more than 42.7% of the student’s fathers had completed their postgraduate degree.
The majority of the participants (68.3%) were staying in hostels and only 13.7% were staying with parents. Nearly 28.5% started using mobiles at the age of 18 years, 53.1% of students used mobile for the first time when they were in the age of 18–20 years followed by 29.7% participants between the age group of 14–17 years.
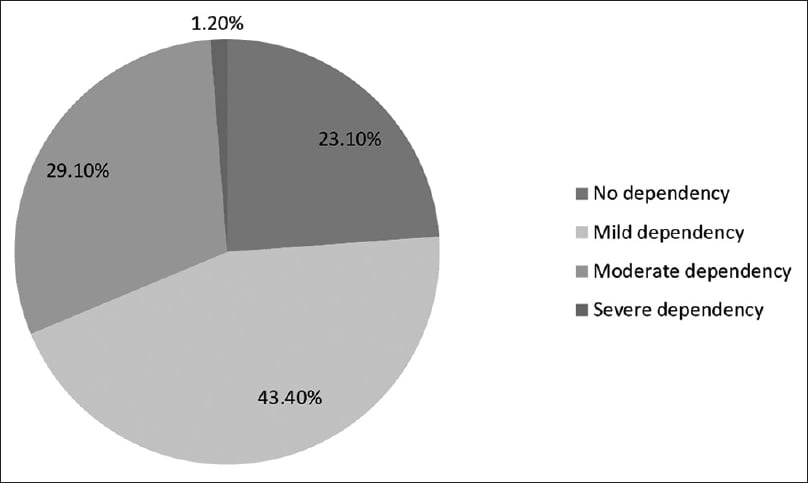
Five percent of the students had severe mobile phone dependency, 29.1% of students had moderate, and 43.4% of students have mild dependence on mobile phones [Figure 1]. Twenty-four percent had mild, 8% had borderline, and 10% had a moderate level of depression. The majority of the students (56%) were normal, whereas 2% had severe depression [Figure 2].
 |
Figure 1: Distribution of students based on the dependence of mobile phone (n = 701)
Click here to view |
 |
Based on the duration of mobile phone usage majority of the students (48.2%) used mobile phone for 1 hour per day and only 18.5 % used mobile phone >2 hours as shown in [Table 1].
| Table 1: Distribution of students based on duration of mobile phone use (n=701) |
The mobile dependency grades across different socioeconomic variables such as age, sex, family type, number of siblings, father’s and mother’s education and occupation, total family income, and monthly pocket money allowances, and residence were assessed. Among them, mother’s occupation had a statistically significant association with mobile dependence (P < 0.05) [Table 2]. There was no significant statistical association seen between mobile phone dependence and depression [Table 3].
 |
Table 2: Association between Socio demographic variables and mobile dependency |
Discussion |
Mobile phone dependence is becoming a major concern among today’s youth. The present study is an attempt to understand android phone dependence among students, to ascertain the factors influencing their use and dependence, and its association with depression.
According to the present study, the prevalence of mobile phone usage was found to be 99.7%, whereas a study done in South India[11] reported a prevalence of 70%. This difference in the prevalence might be due to the difference in the inclusion criteria in both the studies. While majority of the participants in the other study were adults and were females and homemakers, in our study, majority of participants, were adolescents and young adults and were staying in hostels. The experience of boredom, loneliness, and availability of privacy, ease of Internet access, and minimal presence of parental supervision are the factors that likely escalate the excessive use of the Internet. Another study done in South Chennai[12] reported a prevalence of 97%, which is similar to our study with the majority of study participants being college students.
In the present study, only 33.5% had moderate-to-severe mobile dependence, whereas a study done in Chandigarh showed 73.6% moderate-to-severe mobile dependency.[13] The amount of time an individual spends on the Internet is a crucial factor that increases the risk of mobile dependency. Our study findings suggest that majority of the participants used mobile phones for 1 h/day, which was less compared to a study done in South India[11] where the students spent >3 h of Internet usage per day. The difference in the proportion of mobile dependency can be due to the difference in the sociodemographic aspects and access.
In the present study, there was no statistical association seen between mobile phone dependency and depression. A study done by Lemola et al.[14] did not find any association between smartphone usage and symptoms of depression which was similar to our study. Many other studies have shown that there is an association between mobile dependency and depression.[1],[15],[16] A study done by Park et al.[13] shows that moderate use of mobile phones may contribute to improving emotional and psychological well-being. Besides, smartphone communications can be used to relieve stressful situations. The discrepancy can be because most of our study participants were in professional courses who might be using mobile phones for study purposes. Furthermore, the difference might be due to the other studies using different questionnaires and scales for accessing dependency and depression.
There was a significant association between mobile dependence and mother’s occupation in our study, which was similar to a study done in Himachal Pradesh.[17] Few other studies showed a significant association between mobile phone dependency and fathers’ occupation.[18],[19] Parental employment status and unavailability can have an impact on boredom and loneliness with few parental restrictions leading to increased use of the Internet, but a study done by Sharma et al.[19] found that there was no correlation between the working status of both parents and mobile dependence.
In our study, MPDQ was used to assess mobile dependency based on the variables such as the frequency of usage, putting relationships or studies at risk due to excessive use of mobile phones, preoccupation with mobile phone use, and psychological effects such as sleep disturbance. However, there is no mention of mobile phone dependency, however, in the Diagnostic and Statistical Manual of Mental Disorders which does separate behavioral dependency from dependency related to substance use. Hence, there is an existing debate among medical professionals whether to consider cell phone usage as an addiction/dependency or as problematic behavior. At the same time, it is worth noting that there exists few similarities between excessive mobile phone usage and behavioral addiction like gambling as in the loss of control over the behavior, persistence (i.e., having difficulty in limiting the behavior), tolerance (i.e., need to engage in the behavior more often to get the same feeling), and withdrawal (feelings of irritability and anxiety when the behavior is not practiced).[20]
The strength of this study is the large sample size and the limitation would be that the study was done among undergraduate university students, and hence, the results cannot be generalized to the adolescent population necessitating further community-based study in this direction. Furthermore, once the participants were screened for mobile dependency and depression, through questionnaire-based tools, they were not clinically assessed for the confirmation of the same.
We would like to recommend based on the findings of the study as majority of the participants had some degree of mobile dependency to take steps in developing recreational programs for students during the leisure time to maintain students’ mental health, and thereby decrease addiction to a variety of new digital media such as the Internet, chat rooms, computer games, and mobile phones.
[“source=jmhhb”]